See
notes

Here, we outline the objective results of your assessment, the progress towards functional goals and any treatments performed. Include details of any interventions, as well as frequency, duration and equipment used. The therapist should indicate changes in the patient's status, as well as communication with colleagues, family or carers.
S  O A P
O A P

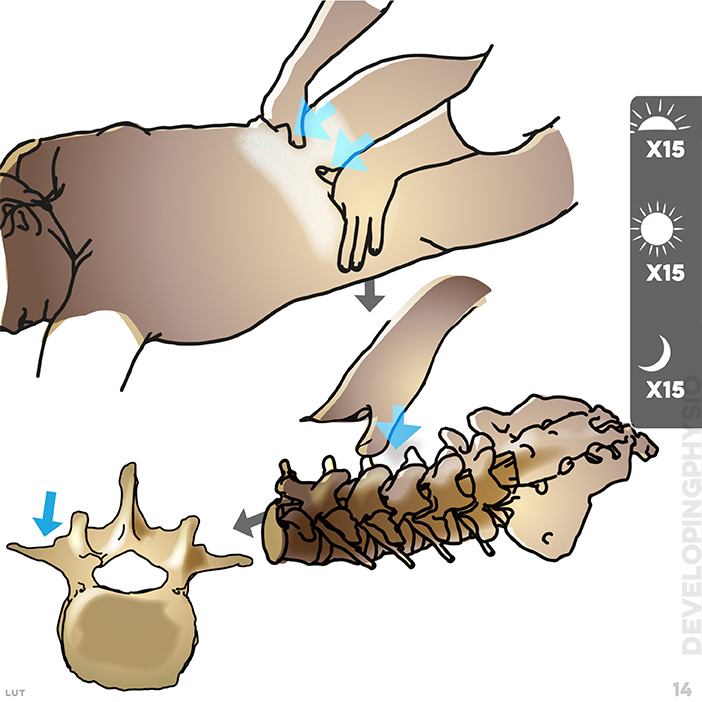
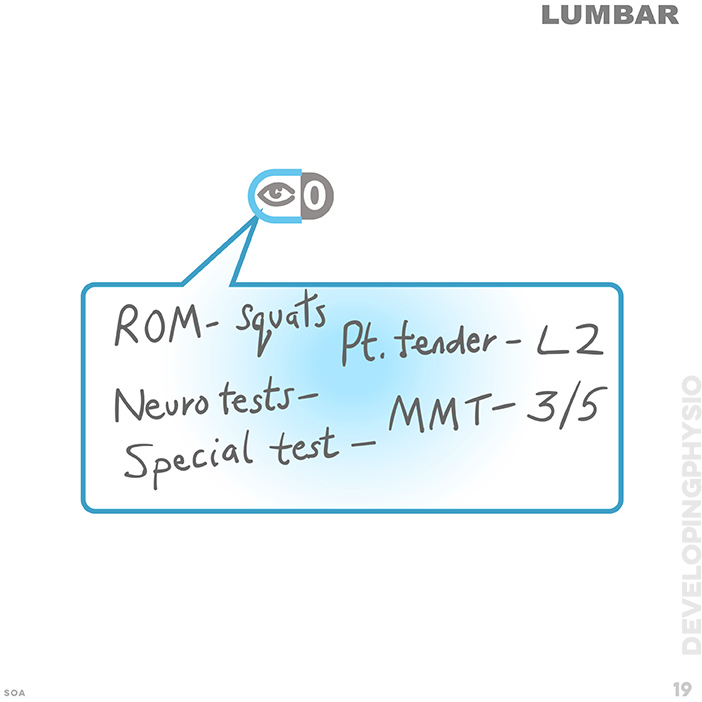
In the second Objective stage of the assessment, the physio makes her/his own observation and evaluation of the patient.
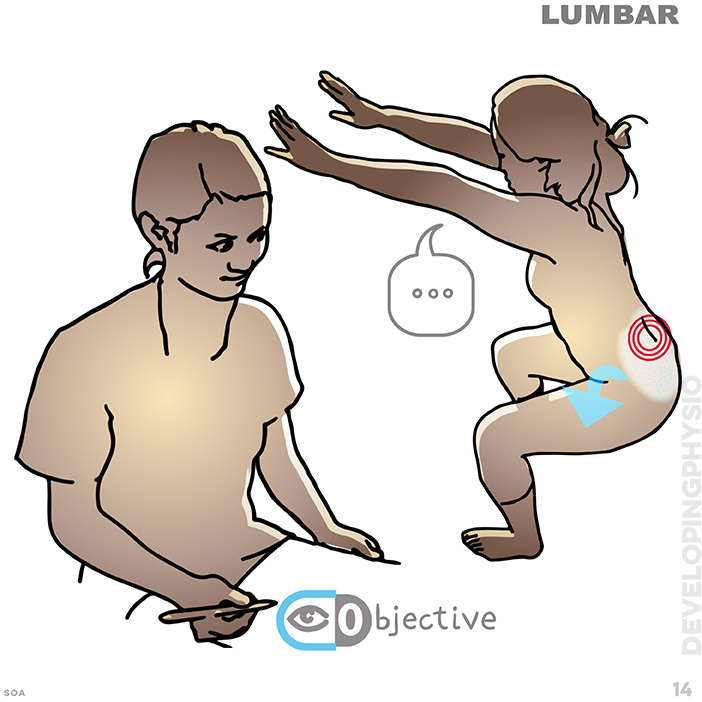

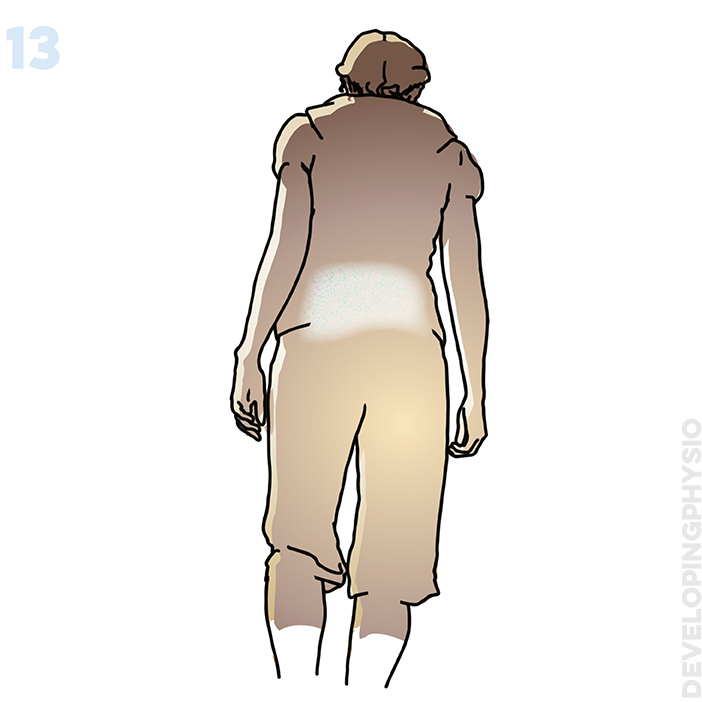
Describe the patients posture
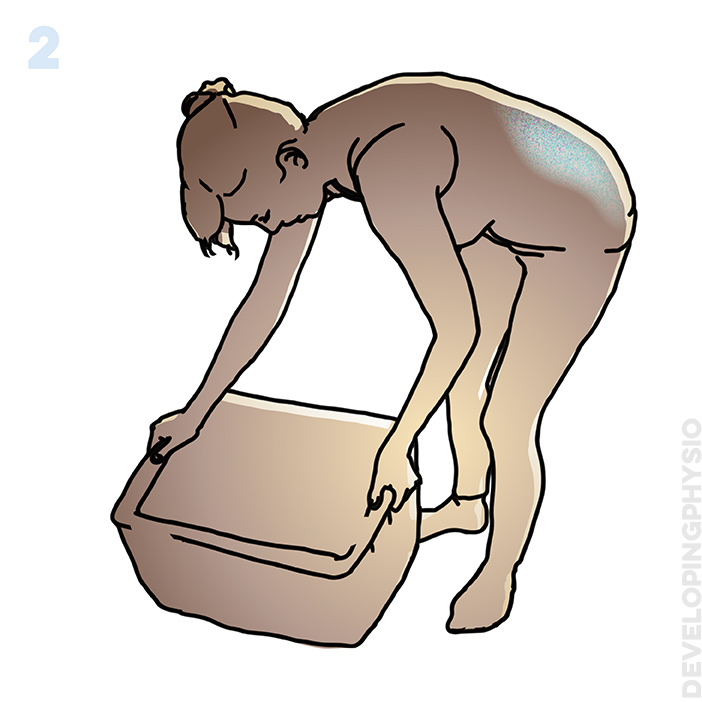
What is their range of motion?
(including passive and active)
Which movements are weak?
What reproduces the pain?

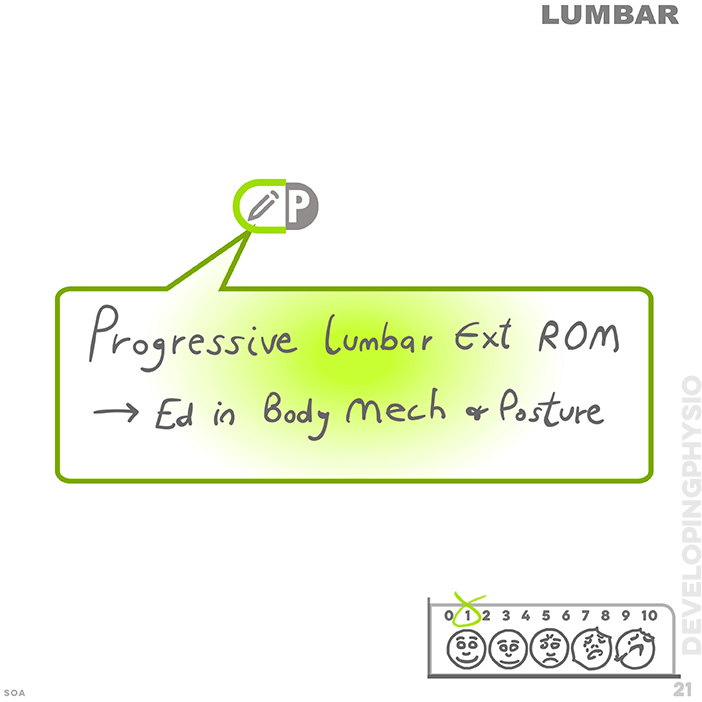
What intervention helped to relieve pain and improve movement?
Try to avoid:
Giving no detail or summary detail such as: "ROM exercises given"
[The Analysis stage now follows] ![]() Analysis
Analysis
Analysis
notes
This is potentially the most important legal note because this is the therapists professional opinion in light of subjective and objective findings. It should explain the reasoning behind all decisions taken and clarify and support the analytical thinking behind the problem-solving process. How you arrived at the stated goals should be indicated, as well as any factors that may require modification, such as frequency, duration or intervention itself. Adverse, as well as positive responses should be documented.
Common errors:
S O A P
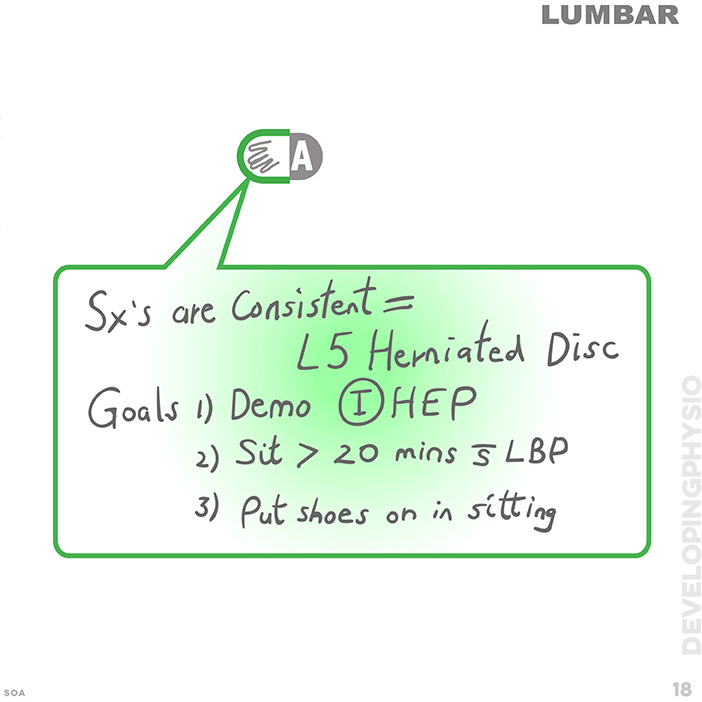
The third Assess stage is an analytical one where the physio further evaluates of the patient.
An assessment note might address the following:
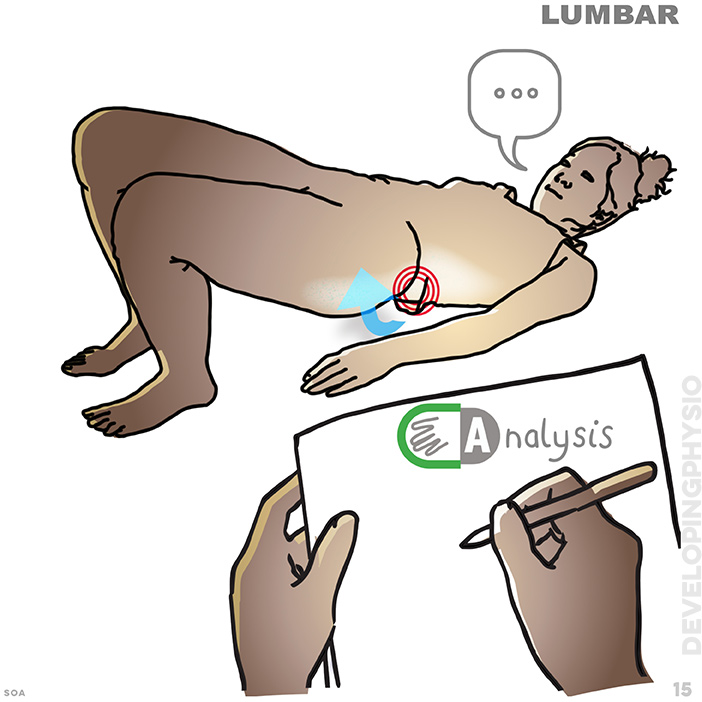

Clinically this might be shown as something like this:
Plan
notes
The final component of the note is used to outline the plan for future sessions. The therapist should report on what the patient's Home exercises will be, as well as the steps to take in order to reach the functional goals. Changes to the intervention strategy are documented in this section.
Common errors:
might need a reminder system here for either a diary system or an 'alarm clock' signal when imminent also an onward referral or discharge tab(? )
S O A P

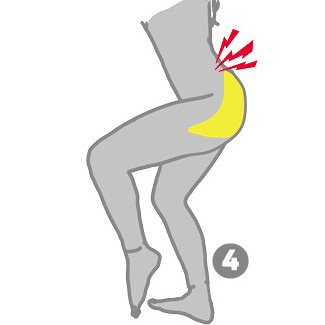
The fourth and final Plan stage is an evaluation of treatment to date.
Typical Plan notes might be
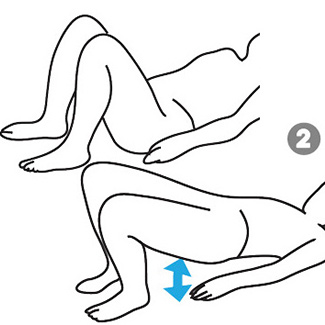
What is the patient’s home exercise program? Crook-lying ADIM 5 sec hold, 10x2, breathing gentle Crook-lying pain-free ROM rotation, breathing gentle

When will he/she return next? Introduce leg movements with abdominal activation
What will you re-assess at the next appointment? re-assess VAS scale
Next appointment? (for patient)
VAS scale?
O A P notes
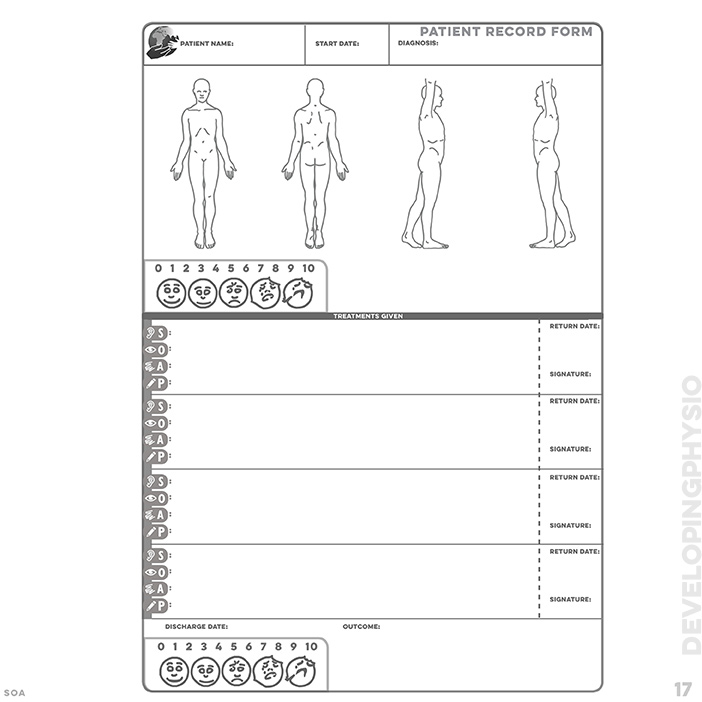
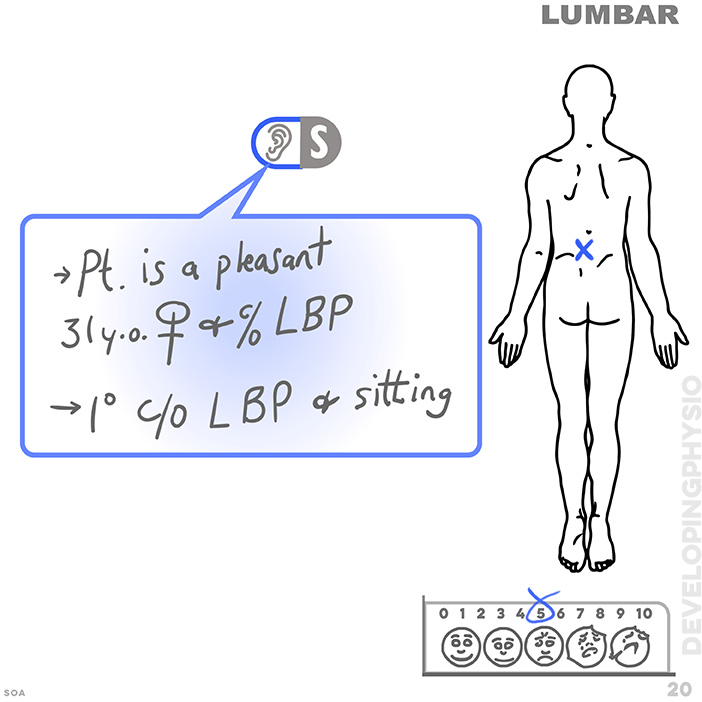
Starting with the Patient Record Form we note down all detail, in the following way
[click any image for gallery]:
And remember, don't:
pass judgement on a patient e.g. "Patient is over-reacting again", and don't document irrelevant information e.g. "patient complaining about previous therapist".